
Every now and then, I am still surprised by what I find in a pet patient’s mouth. This case illustrates that point very well. I am sure you have all been in the same position when asked whether or not a patient should have their teeth cleaned. In some cases, the calculus accumulation is so mild that you really don’t think they are ready for a professional veterinary dental cleaning. I always tell people that you can’t really tell what is going on with a patient’s mouth without veterinary dental radiographs. It is like a broken record I play again and again. But at times, I just don’t feel like a cleaning is warranted. I certainly don’t want to deliver unnecessary care. I almost took that stance with this patient, which would have been a huge disservice to the patient and owner. Of all people, I should know better, but it takes a case like this every now and then to reinforce my beliefs. This case illustrates the fallacy of non-anesthetized pet dental cleanings for veterinary patients. Feel free to share these images with your clients in the exam room, as an example of the importance of an anesthetized exam and veterinary dental radiographs.
“Huey” is a five year old cm miniature dachshund. He had never had his teeth cleaned, but the owners were concerned because they had several other dogs who had required extensive periodontal therapy. In their other dogs, my initial exam had suggested that they might have some issues and that a cleaning, detailed oral exam and dental radiographs were warranted. As most of you are aware, it is common to find more problems that initially anticipated once the teeth are cleaned and dental radiographs are taken.
In Huey’s case, he had almost no visible calculus, no teeth were mobile and he only had a few localized areas of minimal gingival inflammation. I wrestled with whether or not to recommend a cleaning, but I did so for two reasons- first, because he was a small breed dog and second because he was five years old and had never had his teeth cleaned. Pre-surgical CBC and blood chemistry values were all within normal limits.
Huey required 12 extractions and multiple periodontal pockets that required treatment with closed root planing and the placement of Doxirobe gel.
This case illustrates the need for a thorough veterinary oral exam and dental radiographs in every patient. Next time you question recommending professional veterinary dental care for a patient with minimal calculus that has not had a cleaning for over a year, take another look at these pictures and radiographs, share them with the owner, and be an advocate for the patient by recommending good professional veterinary dental care.
Follow Huey’s story in the images below.

Left lower side prior to cleaning. Almost no calculus is visible.

Right lower side prior to cleaning. Essentially, no calculus is visible. Would you recommend a cleaning for this patient based on this picture?

Right upper side prior to cleaning. Not much exciting here either.

Left upper side prior to cleaning. Focal areas of mild gingivitis can be appreciated around 207 and 208. This was the most severely effected area noted on the initial oral exam, but I was not very concerned.
Now it gets interesting! The dental radiographs and anesthetized oral exam revealed some surprising pathology. Note that without an anesthetized exam and veterinary dental radiographs, none of this would have been identified.
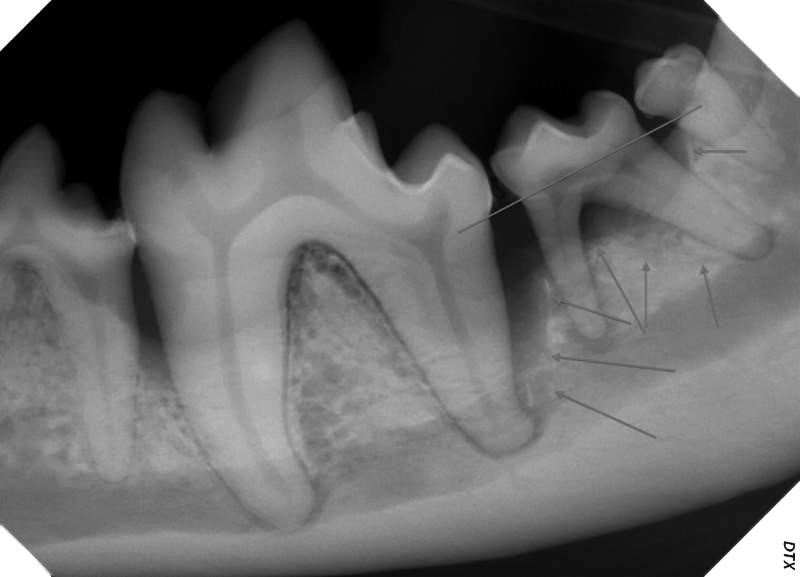
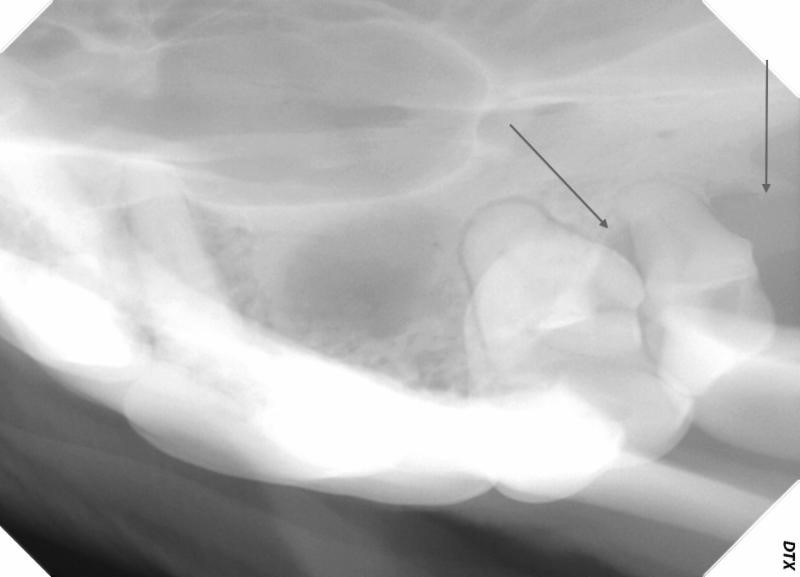
Dental radiograph of 308-311, showing severe bone loss around all of these teeth. Go back and look at this picture of this area above. The straight line shows the approximate normal bone level. The arrows show the areas of severe bone loss. This was a periodontal pocket approximately 14 mm deep! It is not possible to clean this in an unanesthetized patient.
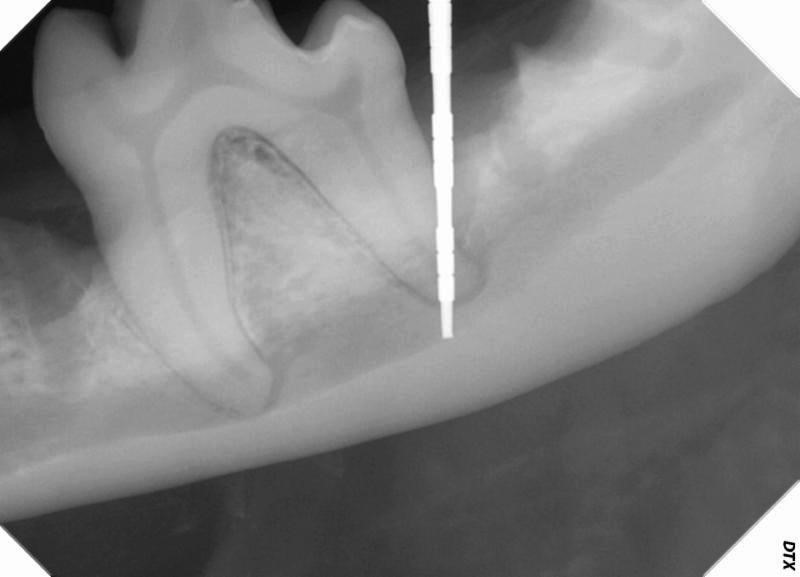
A periodontal probe could be placed to the apex of the distal root of 309, which means that the tooth is likely endodontically infected secondary to bacterial ingress via the apical delta canals. This tooth is a poor candidate for periodontal therapy. The tooth could be treated, however, with a hemi-section, extraction of the distal root and root canal therapy of the mesial root. This treatment would maintain most of the chewing function of the tooth.
After extraction, a bone graft material (Fusion- Veterinary Transplant Services) was placed in this large defect to help stimulate bone growth. The site was curetted and thoroughly lavaged prior to placement of the graft material.

After extraction of 308/309/310/311, showing the absorbable suture material.

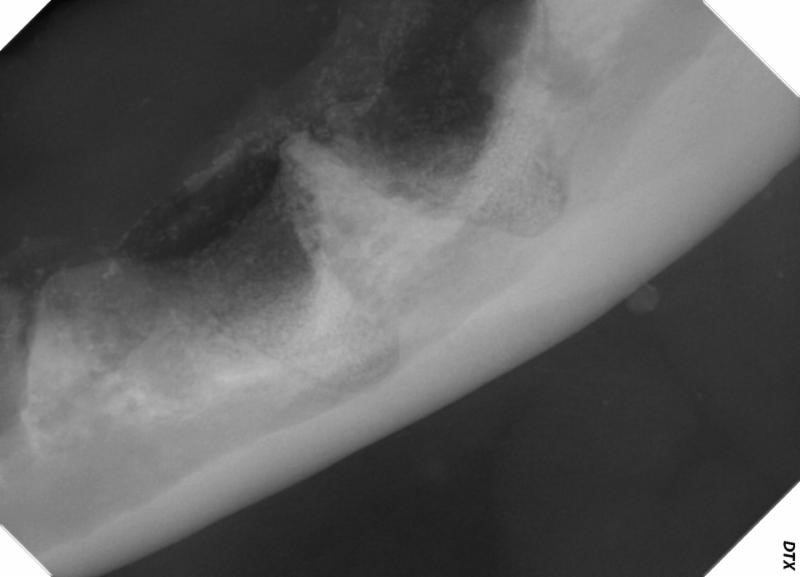
Right lower side, showing dramatic bone loss around 409, 410 and 411. No mobility was present around any of these teeth. Take another look at the pictured of this area above.

Right upper side showing the bony defect around 106, which had a grade 3 furcation exposure.
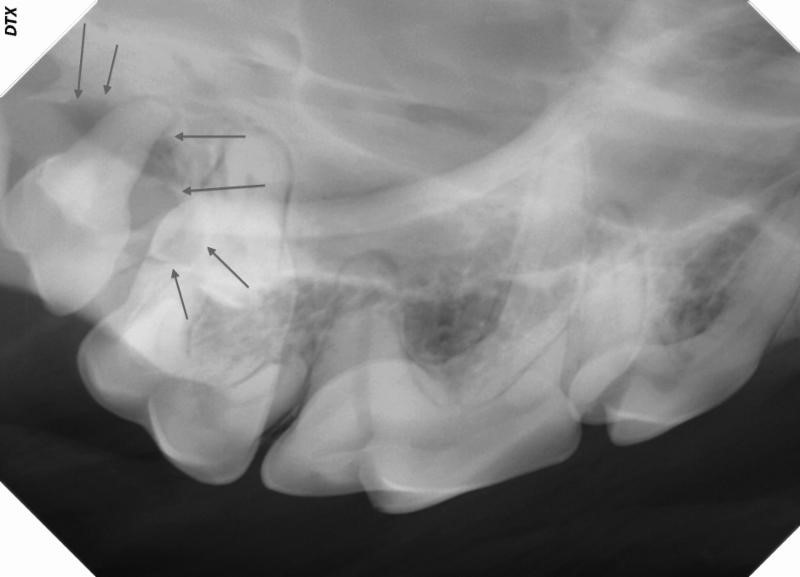
Right upper side, showing bone loss around 109 and 110. 110 had only Grade 1 (slight) mobility despite only having only a small amount of bone remaining around just one of the three roots.
Left upper side, showing similar changes around 209 and 210.